Ignored Warnings and Kentucky’s Drug-Related Diseases

When we think about drug and alcohol addiction and the drug crisis in general, odds are our thoughts and minds go instantly to the death toll of drug use and the families harmed by such losses. And that makes sense. Drug use cannot do more significant harm than claim the lives of those who struggle with such habits.
But what a lot of people do not realize is that many additional problems are brought on as a result of drug abuse. Ignoring these issues is very dangerous because the widespread effects of drug use can sometimes be even more dangerous than the drug use itself.
That might be hard to imagine, but bear with me. One example is the proliferation of sexually transmitted diseases. We’re talking about serious viral illnesses like HIV/AIDS, hepatitis C, and hepatitis A. What many people don’t know is that the transmission of these diseases can occur not only through sex, but also by the sharing of IV drug use needles. In fact, in some instances and locales, these diseases are more likely to be spread via drug use as opposed to sexual contact.
A Drug-Fueled Hepatitis A Outbreak
According to a March issue of USA Today, in the state of Kentucky, 44 people have now died from hepatitis A—one of the dire results of the nation’s largest hepatitis A outbreak. The national outbreak was first declared in November 2017, when 4,288 people were diagnosed with the illness, and 2,065 people went to hospitals to seek help for the condition. Experts insist that the surge of hepatitis A infections is directly connected to a similar rise in IV drug use during that same period.
Hepatitis A is a curable but infectious liver virus. It can be transmitted either by sexual relations with an infected individual or by sharing blood with an infected individual (as in the case of sharing IV needles with an infected user). Hepatitis A does not have to be lethal. There is a vaccine for it, yet many people have died from it in recent years.
In Kentucky at this time, 104 of the state's 120 counties have reported hepatitis A outbreaks among their residents. Medical reports indicate that the majority of these cases were the result of intravenous drug use. The state of Kentucky has not yet declared this situation a medical emergency, but the state’s government has taken steps to fund increased vaccine programs and other emergency-like efforts to curb the increase in hepatitis A cases.
Why Kentucky?
A study featured in the Lexington Herald Leader focused on how eight counties, all of which are in Kentucky, had the most significant decline in life expectancy in the entire nation. Not only that, but these eight counties have maintained that trend from 1980 until 2014. The county with the most significant drop in life expectancy was Owsley County with a decline of 2.3 years. Following were Lee, Leslie, Breathitt, Clay, Powell, Estill, and Perry counties.
Let’s put this into perspective. According to the article, infants born in these eight counties can expect to live shorter lives than their parents. The research attributes multiple factors to such an ongoing and consistent reduction in life expectancy, but it’s generally accepted that obesity, smoking, inactivity, drug use, heavy drinking, poverty, and lack of access to health care are significant factors.
Those factors are breeding grounds for health epidemics. And when drug abuse is entered onto the scene (a health epidemic of its own), other health epidemics are sure to follow. What’s upsetting about the crisis in Kentucky is that these factors have been known for some time—yet insufficient effort has been taken to address them.
“After nearly 200 HIV cases were diagnosed in one southern Indiana community (Austin, Indiana) the CDC conducted a vulnerability assessment of counties most at risk of a rapid HIV spread through people who inject drugs…”
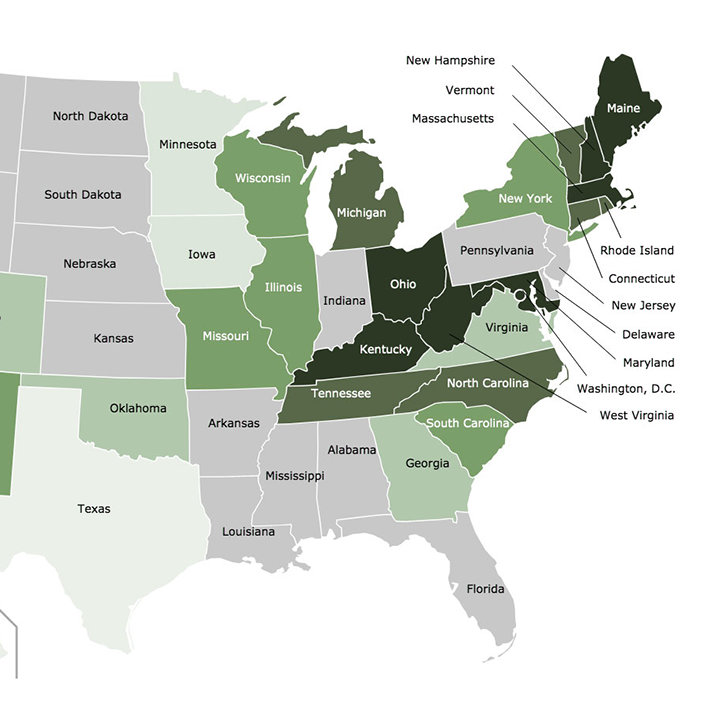
For example, according to WKYT News, “After nearly 200 HIV cases were diagnosed in one southern Indiana community (Austin, Indiana) the CDC conducted a vulnerability assessment of counties most at risk of a rapid HIV spread through people who inject drugs. Of the top 220 counties listed in the report, 54 of them are in Kentucky, and more than half are located in the Appalachian regions of Kentucky, West Virginia, and Tennessee.”
I wrote about the HIV outbreak in Austin, Indiana in an earlier article. But the threat for similar outbreaks is worse in Kentucky. This state needs an emergency-level approach to the drug problem and their health condition overall.
What Can We Learn from This?

What can we learn from the situation in Kentucky? What can we change in our methodology to prevent situations like this from happening in the future?
The health crisis in Kentucky affords us a good lesson. It teaches us that drug overdose deaths are not the only significant risk brought to bear when someone uses drugs. Drug users are not only a danger to themselves, but they’re a danger to others as well.
If an IV drug-user contracts hepatitis A via needle sharing with another addict, he or she will likely be unaware that they even have the disease. And what happens when that drug user has sexual relations with someone else? Possibly someone who does not even use drugs? Now the hepatitis A is transferred once more and is, again likely unknown by either party.
The lesson from Kentucky serves as a grim reminder of two things:
- We need to do everything we can to prevent drug use in our communities.
- If drug use does become an issue, we have to do everything within our power to help those affected to come down off of their grueling habit with the help of residential addiction treatment centers.
Prevention and rehabilitation are our greatest strengths when it comes to tackling the drug crisis. We have to apply prevention by educating our family members, loved ones, and members of our community as to why they would not want to experiment with drugs, in the first place.
And if we know someone who is struggling with a drug habit, we have to do our best to get them into a residential treatment center. We need to do this not only for their well-being, but also so they don’t create a further risk to others in the community. All of this may seem like a daunting task, but having a society which is sober and drug-free—and free of drug-related diseases—is more than worth it.
Action is being taken in Kentucky to curb the state’s health crisis, yet most don’t believe enough is being done. And at the end of the day, we can’t rely exclusively on state and federal governments to solve our problems for us. There comes a time when we all have to work on the improvement of our communities. That time is now.
Sources:
- https://www.usatoday.com/story/news/kentucky-hepatitis-outbreak-death-toll-rises
- https://www.kentucky.com/news/state/
- https://www.wkyt.com/content/news/Report-ranks-54-Kentucky-counties-at-highest-risk-for-HIV-through-needle-injections
Reviewed by Claire Pinelli, ICAADC, CCS, LADC, RAS, MCAP